
Type 1 diabetes – how to control your blood sugar with fewer carbs
While type 1 diabetes requires life-long insulin injections, that doesn’t mean lifestyle can’t still help. In fact, nutrition and exercise may be the key ingredients to managing diabetes better and potentially avoiding the dreaded long-term complications. Read on to learn more!
Type 1 diabetes results when the body is not able to produce the hormone insulin. Insulin keeps blood glucose (sugar) levels under control by helping glucose move from the bloodstream into the body’s cells, where it is used as energy. Because there is a lack of endogenous (self-produced) insulin in type 1 diabetes, this condition is treated with insulin injections, usually multiple times each day.
There is a direct relationship between carbohydrates and the need for insulin. The more carbohydrates a person with type 1 diabetes eats, the more insulin they will need to inject. It should come as no surprise, therefore, that studies and clinical experience show low-carb diets can be beneficial for people with type 1 diabetes.
However, there are special considerations that people with type 1 diabetes need to be aware of when adopting a low-carb diet. Here is our guide to low-carb diets in type 1 diabetes.
This guide is written for adults with type 1 diabetes.
For other controversies related to low carb, see our full guide
What is type 1 diabetes, and how does it differ from type 2?
Type 1 diabetes is an autoimmune disease that destroys the insulin-producing cells of the pancreas, known as beta cells.
By contrast, type 2 diabetes is typically diagnosed after years of insulin resistance, during which the body does not use insulin properly. Early in the process, the pancreas attempts to overcome this resistance by putting out more insulin, which does work to keep blood sugars normal – for a while. Eventually, however, the beta cells begin to fail, insulin levels drop, and the pancreas can no longer put out enough insulin to overcome the resistance and maintain normal blood glucose levels. Once blood sugars rise, the diagnosis of type 2 diabetes is made.
In both types of diabetes, glucose accumulates in the bloodstream, as it cannot enter the body’s cells due to the absence of insulin (type 1) or resistance to and deficiency of it (type 2). Without treatment, blood glucose levels remain elevated, which over time may cause damage to many parts of the body.
Unlike type 2 diabetes, which can often be managed by diet and other lifestyle modifications, people with type 1 diabetes need to inject insulin every day to cover the food they eat. But they also need a source of insulin even when not eating.
This is because the liver continually releases a small amount of glucose into the bloodstream between meals and overnight, to ensure there is enough available for the body’s needs. This process is controlled by insulin. Without insulin, the liver would constantly release large amounts of glucose into the bloodstream, and that glucose would not be able to get into the body’s cells.
Most people with type 1 diabetes are treated with a basal-bolus insulin regimen. This requires injection of long-acting “basal” insulin once or twice daily to keep the release of glucose from the liver under control.
It also requires injecting fast-acting “bolus” insulin just before each meal. Ideally, the dose will vary according to the amount of carbohydrate in the meal, typically by using an insulin-to-carbohydrate ratio (ICR), such as 1 unit of insulin for every 10 grams of carbs.
As for other treatment regimens, few people with type 1 diabetes are treated with two injections a day of mixed (intermediate-acting and fast-acting or intermediate-acting and short-acting) insulin. This does not allow the flexibility of a basal-bolus regimen and usually requires a more standardized meal pattern to maintain stable glucose levels. Others wear pumps that deliver pre-programmed amounts of basal and manual doses of bolus insulin throughout the day. Nowadays, “partial closed-loop systems” are popular, in which a continuous glucose monitor “tells” the pump how much basal insulin to deliver based on blood sugar levels, while the boluses for meals must still be controlled by the user.
Type 1 diabetes used to be called “juvenile diabetes” or “juvenile-onset diabetes” because it is typically diagnosed in children and young adults. However, it can develop at any age, including in the elderly. The oldest person reported to have been diagnosed with type 1 diabetes was a 94-year-old woman.
In older adults, autoimmune diabetes often involves a more gradual destruction of beta cells. This slow, progressive form of diabetes is known as latent autoimmune diabetes in adults (LADA). People with LADA may still produce some insulin, especially when first diagnosed. However, they will eventually require insulin injections in order to control their blood glucose, just like people with type 1 diabetes.
Videos about type 1 diabetes
![How to avoid complications of type 1 diabetes]()
- MEMBERS ONLY
![Carbs or not for type 1 diabetics?]()
- MEMBERS ONLY
![Get off the type 1 diabetes roller coaster]()
![A revolutionary treatment of type 1 diabetes]()
- MEMBERS ONLY
![Treating type 1 diabetes: fact vs fiction]()
![Improve type 1 diabetes with low carb]()
- MEMBERS ONLY
![Treating type 1 diabetes with a keto diet]()
- MEMBERS ONLY
![Low carb or low fat for type 1 diabetes?]()
![Diet Doctor Podcast #37 – Dr. Jake Kushner]()
![How Zein manages type 1 diabetes with low carb and exercise]()
- MEMBERS ONLY
![Managing type 1 diabetes with low carb with Dr. Katharine Morrison]()






What are the risks of type 1 diabetes?
People with type 1 diabetes are at increased risk for a number of health issues, including heart disease, kidney disease, loss of vision, nerve damage and amputations.
Importantly, these risks are linked to having high blood glucose levels, not simply having diabetes.
The American Diabetes Association has set the following blood sugar targets for people with diabetes who are otherwise healthy:
- Fasting blood glucose: 80-130 mg/dL (4.4 – 7.2 mmol/L)
- 2-hour postprandial (post-meal) blood glucose: less than 180 mg/dL (10 mmol/L)
- HbA1c: less than 7% (53 mmol/mol)
These numbers are quite a bit higher than what are considered healthy values for people without diabetes. Healthy people typically have fasting blood glucose levels below 100 mg/dL (5.5 mmol/L) and rarely experience blood glucose above 140 mg/dL (7.8 mmol/L) after eating.
Additionally, a normal HbA1c is considered 5.7% (39 mmol/mol) or less.
However, the DCCT trial, which followed more than 1,400 people with type 1 diabetes for nine years, demonstrated that maintaining an HbA1c level of 7% (53 mmol/mol) or less was associated with a low risk of diabetes complications.
But achieving very tight diabetes control in the DCCT trial was linked to an increased risk of hypoglycemic episodes. Clearly, at least part of the reasoning behind ADA’s more generous targets for blood sugar and HbA1c is to avoid dangerous lows.
However, this assumes that the only way to reduce blood glucose is by giving more insulin. Yet if you are eating a low-carb diet to manage your diabetes, you will need less insulin, blunting the concern about increased hypoglycemia with more intensive glucose control. In fact, research suggests that a low-carb approach may potentially reduce the risk of hypoglycemia.
Carb counting vs. low carb for type 1 diabetes
Prior to the discovery of insulin in 1921, many doctors placed their patients with diabetes on very-low-carb diets because they recognized that carbs raise blood glucose much more than does protein or fat.
The advent of injectable insulin allowed those with type 1 diabetes to eat carbohydrate without dramatically raising their blood sugar. However, even with insulin, controlling blood glucose levels can be a major challenge for them.
Today, diabetes educators often tell people with type 1 diabetes that they simply need to take insulin to match the amount of carbs they eat at each meal. In fact, many people who use ICRs have repeatedly heard, “You can eat whatever you like as long as you take the right dose of insulin.”
However, there are several issues with this approach, including:
- Mistakes with carb estimation. In one study, the carb content of many foods was frequently overestimated or underestimated by children with type 1 diabetes and their parents – as well as by doctors and dietitians.This risks too much or too little insulin being given.
- No differentiation between types of carbs. Slowly digested carbs (such as vegetables) can raise blood sugar less and more gradually than rapidly digested carbs (like white bread).
- Does not account for macronutrient composition of meal. Studies in people with type 1 diabetes have clearly shown that the amount of fat and protein in a meal will affect post-meal blood sugars. Specifically, fat is known to blunt the blood glucose rise in the first 2-3 hours and delay the peak glucose level due to delayed gastric emptying. While eating significant amounts of protein without carbs will not affect blood sugars, protein eaten with carbs will result in a higher peak blood glucose than that same amount of carbs without protein.
- Does not take insulin absorption variability into account. Researchers have shown that the amount of insulin absorbed from an injection may vary by as much as 25% in the same person.
For many people with type 1 diabetes, eating high-carb foods and taking large doses of insulin can cause blood sugar levels to resemble a rollercoaster rather than remaining within a narrow range.
In his book, Dr. Bernstein’s Diabetes Solution, Dr. Richard K. Bernstein explains that eating very small amounts of slowly-digested carbs and taking very small doses of insulin leads to more predictable results and essentially normal blood sugar levels. He calls this “The Law of Small Numbers.”
This makes a lot of sense, doesn’t it? Let’s say you estimate that a meal of meat and broccoli contains 25% fewer carbs than it actually has (for example, you estimate the meal to have 8 grams of carbs but it actually has 10 grams). You take a dose of insulin that would cover 8 grams of carbs, so you have only 2 grams of carbs that is not covered. Your blood glucose would rise only slightly more than if you had been able to exactly match your carb intake and insulin dosage.
Underestimating the carb content of a high-carb meal by 25% can lead to a very different outcome. Many people would consider meat, broccoli, potatoes, milk, and fruit a “healthy” diabetic meal. However, if you take a dose of insulin to cover an estimated 60 grams of carbs rather than the 80 grams this meal actually contains, you’re likely to experience high blood glucose.
Overestimating the carb content of a high-carb meal creates a more urgent concern. Taking significantly more insulin than needed for a high-carb meal may result in hypoglycemia – dangerously low blood glucose that requires immediate treatment to prevent potential loss of consciousness.

Research supporting low carb for type 1 diabetes
Carb restriction for diabetes has mainly been studied in people with type 2 diabetes. However, results from the few studies that have tested this approach in people with type 1 diabetes demonstrate that it can be very effective for them as well:
- In 2016, a small randomized, controlled trial (RCT) found that people with type 1 diabetes who limited carbs to 75-100 grams per day for 12 weeks had significant reductions in HbA1c and blood glucose levels compared to those who practiced standard carb counting. Additionally, those who were overweight showed a non-statistically significant trend toward weight loss (11 pounds or 5kg).
- In 2021, a RCT found that a low-carb/high-protein diet led to less glycemic variability and hypoglycemia.
- In 2019, another small 12-week RCT showed that when 10 people with type 1 diabetes consumed fewer than 100 grams of carbs per day for 12 weeks, they achieved more stable blood sugar levels and had fewer episodes of low blood sugar than when they ate 250 grams of carbs per day. What’s more, they lost about 5 pounds (2 kg) during the low-carb phase and gained almost 6 pounds (2.6 kg) during the high-carb phase.
- In 2017, a shorter RCT found that people with type 1 who ate fewer than 50 grams of carbs per day for 1 week experienced more stable blood sugar control and fewer hypoglycemic episodes than they did during a week of eating 250 grams of carbs and the same number of calories per day.
- In 2018, a group of doctors and researchers published results from a survey completed by 316 people with type 1 diabetes or parents of children with type 1 diabetes who consumed roughly 30 grams of carbs per day. The group reported exceptional blood glucose control with infrequent hypoglycemic episodes and an average HbA1c of 5.67% (39 mmol/mol).
- In 2005, Swedish physicians published the results of an educational program for their type 1 diabetes patients that involved consuming 70-90 grams of carbs per day. They reported significant improvements in HbA1c levels, reduction in insulin dosages, and much more stable blood sugar levels throughout the day. One of the most impressive findings was a 94% decrease in hypoglycemic episodes after 3 months and an 82% decrease at 12 months.
![Blood sugar before and after starting a low-carbohydrate diet]()
![Blood sugar before and after starting a low-carbohydrate diet]()
![Blood sugar before and after starting a low-carbohydrate diet]()
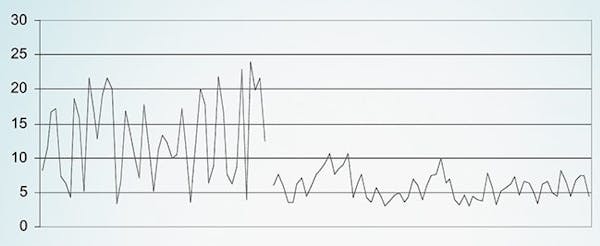 Blood sugar before and after starting a low-carb diet [ref]
Blood sugar before and after starting a low-carb diet [ref] - In 2011, the same doctors reported that the patients in their program who remained consistently low-carb maintained excellent blood sugar control with an average decrease in HbA1c of 1.8% after four years.

Low carb and type 1 diabetes
How many carbs should someone with type 1 diabetes eat every day?
The short answer is that optimal daily carb intake varies among people with type 1 diabetes. As shown in the studies above, restricting carbs to fewer than 100 grams daily is often sufficient to improve blood sugar control and reduce the risk of severe hypoglycemia.
However, a very-low-carb approach (less than 30 grams per day) will require the least amount of insulin, possibly resulting in even more predictable blood sugar control and a greater likelihood of remaining within the healthy range throughout the day and night.
How people with type 1 diabetes can safely achieve great blood sugar control with low carb
People with type 1 diabetes who want to start eating low carb should ideally work with a doctor, nurse, dietitian or other health professional who specializes in diabetes and understands carb restriction.
This is because, in addition to decreasing the amount of insulin you take to cover carbs, you may need to make other adjustments, such as reducing your basal insulin dosage. Although the principles of management apply to everyone, you will need to assess the effects of a low-carb diet on your body chemistry. The best and safest approach is one that includes frequent testing, keeping detailed records, and evaluating your results.
For people who use an ICR to calculate their mealtime insulin doses, it is easy to manage a low-carb diet because the ratio will remain the same. So as you eat fewer carbohydrates, you will naturally inject less insulin.
Some overweight people will lose weight with a low-carb diet and become more insulin sensitive. If this occurs, it may be necessary to reduce the ICR, and probably also the basal insulin doses.
Protein may also need to be accounted for when calculating insulin dosage at mealtimes. Studies show that adding protein to a meal that contains carbohydrate will contribute to a higher peak glucose level.
Failing to account for protein may result in excellent blood glucose levels an hour or so after a meal but higher levels several hours later.
As with carbs, insulin dosing for protein intake varies from person to person, and determining your own body’s needs will take some experimentation. If you underestimate the amount of insulin needed at a meal, the higher post-meal blood glucose can be managed by taking a correction dose of insulin at the next meal.
Alternatively, short-acting insulins (regular insulin) can be used with high-protein meals. These insulins have a slower onset of action than rapid-acting insulin analogs (such as aspart, lispro, and glulisine).
In one of his Diabetes University videos, Dr. Bernstein provides an excellent discussion about how to cover protein with insulin.
Additionally, his books and online resources provide more in-depth and individualized guidance for those who have type 1 diabetes and want to transition to a low-carb lifestyle safely.
Learn more about insulin dosage on a low-carb diet

Success stories
![How Leonie successfully manages type 1 diabetes]() How Leonie successfully manages type 1 diabetes
How Leonie successfully manages type 1 diabetes!["Overall, I now have a completely new life"]() "Overall, I now have a completely new life"
"Overall, I now have a completely new life"!["I still have 30 pounds to lose, but I've already won"]() "I still have 30 pounds to lose, but I've already won"
"I still have 30 pounds to lose, but I've already won"



Low-carb type 1 diabetes support and resources
Information
Dr. Bernstein’s Diabetes University
Dr. Bernstein’s Diabetes Solution (Read several chapters of his book online)
Take Control of Type 1 Diabetes (Book by Dr. David Cavan)
Individualized guidance from type 1 health professionals
Ketogenic Diabetic Athlete (Dr. Keith Runyan)
SVV Nutrition (Sean Vander Veer, Registered Dietitian)
Kelly Schmidt Wellness (Kelly Schmidt, Registered Dietitian)
DiaVerge Diabetes (Lisa la Nasa, Certified Level 2 Diabetes Paraprofessional)
Community/Forum
Podcast and videos
Diet Doctor Podcast #37: Dr. Jake Kushner
Video: Dr. Jake Kushner: Low fat or low carb for type 1 diabetes?
Video: Managing type 1 diabetes with low carb with Dr. Katharine Morrison
Low carb: benefits and limitations
It cannot be overemphasized that many things besides food can affect blood glucose levels, including stress, illness, increased physical activity and even seemingly mild alterations in sleep. Most of these are difficult or even impossible to prevent. Therefore, the most important thing when it comes to managing type 1 diabetes is to understand how these things can affect your glucose control.
If it is something you can predict, such as planned increased activity, then you can make adjustments to your insulin dose. If not, then it is important to know how to respond to an unexpected low or high glucose reading. Frequent testing is key and makes it much easier to manage these effects.
Fortunately, a low-carb diet can help you avoid big changes in glucose levels related to food, and simplifies mealtime insulin dosing so that a huge piece of the diabetes puzzle is no longer an issue. This can significantly improve your overall diabetes control, reduce anxiety, and enhance your quality of life.



Learn more about type 1 diabetes
![How to avoid complications of type 1 diabetes]()
- MEMBERS ONLY
![Carbs or not for type 1 diabetics?]()
- MEMBERS ONLY
![Get off the type 1 diabetes roller coaster]()
![A revolutionary treatment of type 1 diabetes]()
- MEMBERS ONLY
![Treating type 1 diabetes: fact vs fiction]()
![Improve type 1 diabetes with low carb]()
- MEMBERS ONLY
![Treating type 1 diabetes with a keto diet]()
- MEMBERS ONLY
![Low carb or low fat for type 1 diabetes?]()
![Diet Doctor Podcast #37 – Dr. Jake Kushner]()
![How Zein manages type 1 diabetes with low carb and exercise]()
- MEMBERS ONLY
![Managing type 1 diabetes with low carb with Dr. Katharine Morrison]()