




High protein diet:
What it is and how to do it
You may have heard that high protein diets can help with weight loss and metabolic health. That’s why, at Diet Doctor, we feature high protein recipes and meal plans. But how do you know if a higher protein diet is right for you?
This guide will explain what high protein diets are, help you find the best high protein foods, and explore the potential benefits of high protein diets.
Key takeaways
What are the best high protein foods?Meat, seafood, eggs, beans, and dairy are all great sources of protein.
Find out if your favorite foods are also high protein.
What can high protein do for you?
You can lose weight, improve your health, and gain muscle by adding protein to your diet.
Learn more about how high protein could benefit you.
How much protein do I need?
More than you probably think! But it’s easy to add more protein to your diet with a few simple tricks.
Find them here.
1. What is a high protein diet?
A high protein diet is one where you work on getting plenty of protein — probably more than you are used to getting — as the first focus of your eating patterns. Protein-rich foods include eggs, meat, seafood, legumes, and dairy products. These foods are not only high in protein but high in nutrients in general. That means a high protein diet is also a high nutrition diet.
Increasing protein can be very helpful for weight loss because protein can help tame your appetite.1 It also supplies plenty of the raw materials needed to maintain your muscles and your metabolism, both of which help ensure that you’re burning calories at an appropriate rate.2
For people who want to build muscle, getting more protein than is typically recommended is a must. Current recommendations, known as the RDA or the recommended dietary allowance, are designed for “healthy people” and meant to prevent malnutrition; they aren’t meant to help increase muscle mass or improve medical conditions such as type 2 diabetes.3
Diets with increased protein can have a positive effect on the treatment and prevention of type 2 diabetes and metabolic syndrome, and possibly even heart disease.4 Higher protein intake also helps prevent sarcopenia, which is a loss of muscle mass that can occur as you age, and a related condition, osteoporosis, which is a loss of bone mass.5
More high protein guides





More high protein guides

You can read more about how much protein most people are eating now in our expanded section here:
2. What are the best high protein foods?
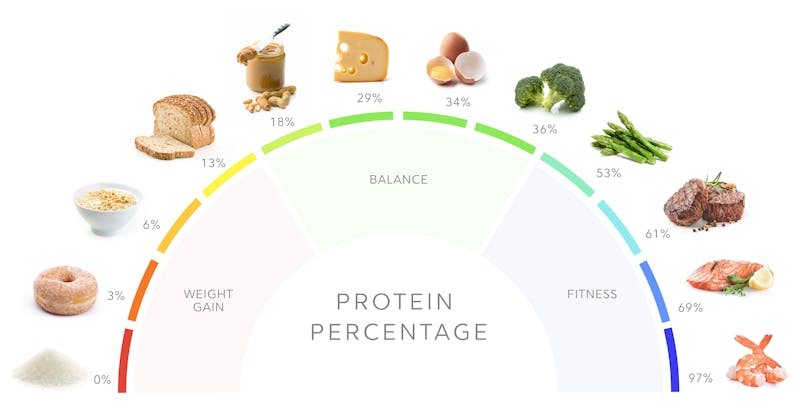
The best choices for high protein diets are foods with a high protein percentage. The protein percentage of a food tells you how much protein per calorie a food has.10 Foods with a lot of protein and less fat and carbohydrate are ranked higher, as are low-fat, low-carb foods with a lot of fiber.
Foods in the middle range of protein percentage can help you maintain your weight and your muscle mass. Going a little higher — over 30 or 35% — may help you lose weight.
Foods with a lower protein percentage may lead to weight gain, while foods with the highest protein percentage may be good choices for someone who is really trying to reduce body fat and become lean and fit.
Fortunately, most high protein foods are delicious and have plenty of vitamins and minerals, too. You can start with this list of the best high protein foods.
- Meat and poultry: beef, chicken, lamb, turkey
- Seafood: shrimp, crab, salmon, tuna
- Eggs: whole eggs or egg whites
- Dairy: cottage cheese, greek yogurt
- Legumes: Beans, lentils, peas, and soy
- Non-starchy vegetables11: spinach, cauliflower, broccoli, mushrooms
If your diet consists mainly of the above foods, you are on your way to eating a healthy diet with plenty of protein.
Remember that non-starchy vegetables may have a high protein percentage, but they won’t give you the total protein, calories, or all the nutrients you need. Base your meals around a protein source — whether from animals or plants — and add high-protein-percentage vegetables for a little extra boost of amino acids, the building blocks of protein. Add just enough fat to make your meals delicious and filling. This approach will keep the total protein percentage of your meals high.
Here are a few tips to help you increase how much protein you eat and ensure you get adequate protein without adding too many unnecessary calories:
- Add extra egg whites to your scrambled eggs or omelets.
- Replace lower protein snacks, like nuts and cheese, with higher protein versions like lupini beans, zero-sugar jerky, or cold cuts.
- Include your favorite foods that are higher than 35% protein. Choose from the highest protein foods such as shrimp, chicken breasts, and lean cuts of meat.
- Swap higher fat cheese and yogurt with low-fat cheese or Greek yogurt. The lower-fat versions have higher protein percentages and therefore more protein per calorie.
You can find the protein percentage of many of your favorite foods and maybe discover a few new favorites, in our guide on the best high protein foods for weight loss.
What about protein powders?
Although our bias is that you should get most of your protein from whole foods, protein powders can still be part of a healthy, high protein diet.
You may not need protein powders if you prioritize the food on our list of best high protein foods. But if you fall short of your daily targets, protein powders are an easy and convenient way to get more protein.
Plus, protein powders are a great way to create high protein versions of your favorite desserts, low-carb bread, or smoothies.
If you are going to use protein powders, make sure they have few additives, such as sweeteners, maltodextrin, seed oils, or fillers.
Animal and plant protein powders are both good options, and you can choose which works best for your taste, preferences, and carbohydrate goals.
Summary
- Foods with the highest protein percentage are low in carbs and fat, like lean meat and seafood.
- To increase the protein in your diet, look for easy substitutions — snack on lupini beans or venison jerky, add two egg whites to your two whole eggs in the morning, or add more meat, seafood, dairy, or legumes to your meals.
- Mix protein foods with high-fiber vegetables – and don’t overdo fat – to create meals with a protein percentage above 35%.
- If you struggle to meet your protein goals with whole foods, consider protein powders.
3. High protein benefits

Weight loss
Multiple studies demonstrate higher protein intake helps with weight loss, specifically fat mass loss.12
Metabolic benefits
Studies show diets higher in protein contribute to better blood sugar control and improved insulin sensitivity when compared to lower protein diets.13 Can eating more protein raise insulin levels in an unhealthy way? Scientific studies don’t support this idea.
While protein may briefly increase insulin concentrations, high protein diets are not known to cause chronic hyperinsulinemia (high insulin levels). In fact, for people with prediabetes or type 2 diabetes, a higher protein diet may be more beneficial than a lower protein one.14
Body composition
Higher protein diets promote lean muscle mass and encourage loss of fat mass.15
Strength, bone health, and preventing frailty
As people age, muscle mass and bone health decline, which, if not corrected, can lead to physical frailty along with an increased risk of falls and bone fractures.16 Eating more protein can counteract this trend toward frailty with improved muscle mass and bone health.17
Satiety
Part of the reason for weight loss and better glycemic control could be protein’s ability to decrease hunger. Numerous studies show that as the protein amount increases, feelings of hunger and the amount of food eaten the rest of the day go down.18
4. How do we define a high protein diet?
Summary: High protein diets are:
- Diets with more than 25% of calories from protein
- Over 1.6 grams of protein per kilo of body weight
- Diets with more protein than the Recommended Daily Allowance (RDA), which is set at 0.8 grams per kilo.
There is no universally agreed-upon definition of a high protein diet, and what you consider “high” may depend on where you start.
At Diet Doctor, we define adequate protein as over 1.2 grams per kilo per day and high protein as over 1.6 grams per kilo per day or above 25% of calories. We recommend that most people aim for 1.6 to 2 grams of protein per kilo or 25-35% of calories from protein to ensure adequate protein intake. And you should aim for the higher end of that range for a high protein diet.
Our definition of high protein is relative to The US Institute of Medicine, which sets 10% to 35% of calories as the acceptable range for protein intake. But it’s likely that you can safely eat much higher than 35% of your calories from protein.19
5. How much protein do I need?
Summary
- Calculate your daily protein goal based on your height, activity level, and health goals.
- We recommend a protein intake of 1.6 to 2.0 grams per kilo of reference body weight.20
- If you are very physically active or taller than 6 feet, consider staying at the higher end of this range.
- Distribute your protein intake throughout the day, with 30 to 40 grams per meal for women and 35 to 50 for men, if you are eating three meals a day.
The first step in eating a higher protein diet is setting your protein targets. We believe most people would benefit by increasing their protein intake to 1.6 to 2.0 grams per kilo per day, or 25 to 35% of daily calories. Use this simple chart to find out what your minimum daily protein target should be, based on your height.21
Minimum daily protein target
| Height | Women | Men |
|---|---|---|
| Under 5’4″ ( < 163 cm) | 90 grams | 105 grams |
| 5’4″ to 5’7″ (163 to 170 cm) | 100 grams | 110 grams |
| 5’8″ to 5’10” (171 to 178 cm) | 110 grams | 120 grams |
| 5’11” to 6’2″ (179 to 188 cm) | 120 grams | 130 grams |
| Over 6’2″ (188 cm +) | 130 grams | 140 grams |
As the chart indicates, you should try to get around 100 grams if you’re a woman and 120 grams if you’re a man of average height and build. Eat more if you’re a man taller than 6 feet (183 cm) or a woman taller than 5’6″ (168 cm) or if you’re very physically active. Eat less if you’re shorter or have a very small frame.22If you are very physically active, over 50 years old, or most of your protein comes from plant sources, we recommend aiming for the higher end of the protein range (above 1.6 grams per kilo per day). This means adding another 20 to 30 grams of protein to the targets above.
If you are physically active, want to achieve very low body fat (less than 10% for men or 20% for women), or regularly practice intermittent fasting, you may want to add even more protein. Since there are no credible data showing harm from very high protein diets of over 2.0 grams per kilo of body weight per day — as we discuss later in this article — you can feel confident in adding more!
Read more about spacing your protein out during the day and whether you need to count calories.
6. Common concerns about high protein diets
According to some scientists and outdated published articles, high protein diets can be harmful to your kidneys, bones, and blood sugar. Some even believe that higher-protein diets lead to higher rates of cancer.23
With respect to kidney health and protein intake, it is well-recognized that people with severe chronic kidney disease should restrict protein intake. Dietary protein will not, however, cause kidney dysfunction in people with healthy kidneys.24
With respect to bone health in older adults, it was previously believed that high protein intake would lead to osteoporosis via inducing chronic metabolic acidosis (too much acid in the blood from the protein). Multiple studies have since failed to show that high protein intake causes loss of bone density and fractures.25 In fact, protein may even help bone health.26
Another concern with a high protein diet — especially for those on a low-carb diet — is that the amino acids in dietary protein could cause a significant rise in blood sugar.27 According to studies, however, the opposite may be true, and increased protein may improve blood sugar.28
With respect to lifespan, data from flies, mice, and other animals suggest that restricting protein may increase longevity, while human data are very weak.29 We need to consume adequate protein to prevent loss of muscle tissue and frailty as we age, so restricting that nutrient in order to increase lifespan may not benefit general health.
High protein diets are safe for most people. The bottom line is, there is no convincing evidence that high protein diets are harmful — although they are not recommended for people who already have severe underlying kidney disease. You can read more in our guides on bone health and kidney health, as well as our guides on red meat and diet and cancer.
Animal versus plant protein
Is all protein the same? No, not really.
Animal proteins are considered complete sources of protein — meaning they supply all nine essential amino acids — whereas all plant sources aside from soy are incomplete.30 This doesn’t mean you can’t get all essential amino acids from plant sources. It simply means you will need to combine different sources, such as beans with nuts or whole grains.
Your body also absorbs animal proteins much better than most plant proteins, meaning you can eat less for the same effective amount of protein. Again, that doesn’t mean you can’t get adequate protein from plant sources. But it does mean you may need to increase your intake goals by 20% or more.31
Lastly, plant sources of protein tend to be higher in carbohydrates than animal sources. If you follow a very low-carb or keto diet, this can make meeting all your goals challenging.
Soy is unique among plant proteins since it is a complete protein and appears to have similar bioavailability, muscle-building effects, and weight loss benefits as animal proteins.32
However, aside from soy, evidence suggests animal protein may be more beneficial for strength and muscle maintenance and may provide a better source of micronutrients, especially from red meat.33
Longevity and chronic diseases
With respect to lifespan, some observational studies have suggested that plant protein may be associated with better longevity, while animal protein may correlate with earlier death.34 Other observational studies have found no difference in mortality between plant and animal protein.35
These observational studies are considered very weak evidence. At this time, we cannot say that there is sufficient evidence to recommend getting most of your protein from either plants or animals. It is our opinion that eating a diversity of plant and animal sources of protein should be considered a healthy diet.
Summary: Animal versus plant proteins
- Animals provide complete proteins with better absorption and muscle-building benefits.
- Plant proteins can be combined to form complete proteins but may contain more calories and carbs per gram of protein.
- The data on longevity and chronic diseases may raise concerns about animal protein, but the majority of human evidence is low-quality and inconclusive.
7. FAQ about high protein diets
We get it. All this new information about protein can be confusing. If you have additional questions about why or how to add more protein to your meals, check out our FAQ with the “Top 20 questions about high protein diets.”
High protein recipes













Learn more about protein
- MEMBERS ONLY
![Why more protein is better]()
![Too much protein is better than too little]()
![Why you shouldn't fear protein on keto]()
- MEMBERS ONLY
![Is fear of protein the new fear of fat?]()
- MEMBERS ONLY
![Insulin, protein and how to slow aging]()

High protein diet: What it is and how to do it - the evidence
This guide is written by Dr. Bret Scher, MD and was last updated on June 19, 2025. It was medically reviewed by Dr. Michael Tamber, MD on May 13, 2021.
The guide contains scientific references. You can find these in the notes throughout the text, and click the links to read the peer-reviewed scientific papers. When appropriate we include a grading of the strength of the evidence, with a link to our policy on this. Our evidence-based guides are updated at least once per year to reflect and reference the latest science on the topic.
All our evidence-based health guides are written or reviewed by medical doctors who are experts on the topic. To stay unbiased we show no ads, sell no physical products, and take no money from the industry. We're fully funded by the people, via an optional membership. Most information at Diet Doctor is free forever.
Read more about our policies and work with evidence-based guides, nutritional controversies, our editorial team, and our medical review board.
Should you find any inaccuracy in this guide, please email andreas@dietdoctor.com.
American Journal of Clinical Nutrition 2008: Protein, weight management, and satiety [overview article; ungraded] ↩
American Journal of Clinical Nutrition 2006: The underappreciated role of muscle in health and disease [overview article; ungraded] ↩
Applied physiology, nutrition, and metabolism 2016: Protein “requirements” beyond the RDA: implications for optimizing health [overview article; ungraded]
The RDA is defined as the “average daily level of intake sufficient to meet the nutrient requirements of nearly all (97%-98%) healthy people.” The RDA for protein is 0.8 grams per kilo of reference body weight, which is a rough approximation of your lean body mass – the part that needs protein. But, as we explain in this guide, that is likely too low for most people who want to improve their health.
↩American Journal of Clinical Nutrition 2008: Protein in optimal health: Heart disease and type 2 diabetes [overview article; ungraded] ↩
American Journal of Clinical Nutrition 2008: Role of dietary protein in the sarcopenia of aging [overview article; ungraded]
American Journal of Clinical Nutrition 2008: Amount of type of protein influences bone health [overview article; ungraded]
↩Institute of Medicine of the National Academies 2005: Dietary Reference Intakes for energy, carbohydrate, fiber, fat, fatty acids, cholesterol, protein, and amino acids [overview article; ungraded]
Journal of the American Dietetic Association 2002: Dietary reference intakes for energy, carbohydrate, fiber, fat, fatty acids, cholesterol, protein and amino acids [overview article; ungraded]
International Journal of Sports Nutrition and Exercise Metabolism 2006: A review of issues of dietary protein intake in humans [overview article; ungraded]
↩Although it is difficult to know what our hunter-gatherer ancestors ate, some scholars estimate they ate between 20% and 35% of their calories as protein. That equates to a range of 100 to 175 grams of protein per day for a 2,000-calorie intake, or up to 260 grams for a 3,000 calorie intake. This total daily protein amount is two to four times greater than the proposed RDA.
NEJM 1985: Paleolithic nutrition. A consideration of its nature and current implications [overview article; ungraded]
American Journal of Clinical Nutrition 2000: Plant-animal subsistence ratios and macronutrient energy estimations in worldwide hunter-gatherer diets [overview article; ungraded] ↩
American Journal of Clinical Nutrition 2018: Protein intake trends and conformity with the Dietary Reference Intakes in the United States: analysis of the National Health and Nutrition Examination Survey, 2001-2014 [observational study, weak evidence]
American Journal of Clinical Nutrition 2008: Current protein intake in America: analysis of the National Health and Nutrition Examination Survey, 2003-2004 [observational study, weak evidence] ↩
The following observational study reported that the average intake is as follows: Animal 46%, dairy 16%, plants 30%, and undefined 8%.
Nutrients 2015: Sources and amounts of animal, dairy, and plant protein intake of US adults in 2007-2010 [observational study, weak evidence] ↩
We don’t include calories from fiber in our calculations, as the number normally is very small, plus fiber generally has positive effects on satiety. ↩
These are high in protein percentage, although low in overall protein amounts ↩
The first study reports improved body composition and weight loss with no reduction in fat-free mass or resting energy expenditure on a high protein diet in overweight women.
Nutrients 2018: Effects of adherence to a higher protein diet on weight loss, markers of health, and functional capacity in older women participating in a resistance-based exercise program [randomized trial; moderate evidence]
The following study, a 12-week intervention in obese women, also reports more significant fat mass loss with a 25% protein diet than a 15% protein diet.
British Journal of Nutrition 2020: The effect of 12 weeks of euenergetic high protein diet in regulating appetite and body composition of women with normal-weight obesity: a randomised controlled trial [randomized trial; moderate evidence]
And the next two examples also report similar results:
International Journal of Obesity Related Metabolic Disorders 2004:
Effect of normal-fat diets, either medium or high in protein, on body weight in overweight subjects: a randomised 1-year trial[randomized trial; moderate evidence]Endocrine, Metabolic, and Immune Disorders of Drug Targets 2020:
Effects of a low carb diet and whey proteins on anthropometric, hematochemical, and cardiovascular parameters in subjects with obesity [nonrandomized study, weak evidence]The last example is a review of RCTs showing better weight loss in those following higher-protein, low-fat, energy-restricted diets compared to lower protein versions of similar diets.
American Journal of Clinical Nutrition 2012: Effects of energy-restricted high-protein, low-fat compared with standard-protein, low-fat diets: a meta-analysis of randomized controlled trials [systematic review of randomized trials; strong evidence]
↩This RCT reports that those following a 27% protein diet compared to 16% had better preservation of lean mass and a better glycemic response despite no difference in weight loss.
Nutrients 2018: Effects of adherence to a higher protein diet on weight loss, markers of health, and functional capacity in older women participating in a resistance-based exercise program [randomized trial; moderate evidence]
This randomized crossover study reports subjects with type 2 diabetes had a more significant reduction in A1c and total daily glucose, fatty liver, and fatty pancreas with a 30% carb/30% protein diet compared to a 50% carb/17% protein diet.
Diabetologia 2019: A carbohydrate-reduced high protein diet improves HbA 1c and liver fat content in weight stable participants with type 2 diabetes: a randomised controlled trial [randomized trial; moderate evidence]
This small RCT reports 100% prediabetes remission with a higher protein diet.
Nutrition, Metabolism, and Cardiovascular Diseases 2020: High protein diet leads to prediabetes remission and positive changes in incretins and cardiovascular risk factors
↩
[randomized trial; moderate evidence]Diabetes care 2003: Amino acid ingestion strongly enhances insulin secretion in patients with long-term type 2 diabetes. [nonrandomized trial; weak evidence] ↩
Nutrients 2019: Dietary protein and muscle mass: translating science to application and health benefit [overview article; ungraded]
Advances in Nutrition 2019: Recent advances in the characterization of skeletal muscle and whole-body protein responses to dietary protein and exercise during negative energy balance [overview article; ungraded]
Nutrients 2018: Recent perspectives regarding the role of dietary protein for the promotion of muscle hypertrophy with resistance exercise training [overview article; ungraded]
↩The following review reports an age-related gradual loss of muscle mass after age 50:
Clinical and Experimental Pharmacology and Physiology 2007: Age-related changes in the structure and function of skeletal muscles [overview article; ungraded]
And the following 14-week intervention study reports that subjects ages 55 to 77, who ate the RDA protein level of 0.8 grams per kilo per day, decreased muscle mass despite not losing any weight.
Journal of Gerontology Biological Science and Medical Science 2001: The recommended dietary allowance for protein may not be adequate for older people to maintain skeletal muscle [randomized trial; moderate evidence]
This review discusses the age-related changes in both muscle and bone.
Physiology 2015: Aging and the muscle-bone relationship
↩
[overview article; ungraded]The following reviews summarize the evidence for this nicely.
Nutrients 2016: Protein consumption and the elderly: What is the optimal level of intake? [overview article; ungraded]
American Journal of Clinical Nutrition 2015: Protein and healthy aging [overview article; ungraded]
The following observational study reports a high association between eating more protein and having less disability with aging.
Journal of the American Geriatrics Society 2019: Protein intake and disability trajectories in very old adults: The Newcastle 85 Study [observational study with HR over 2, weak evidence]
Higher protein intake, especially when eating animal foods, is associated with greater muscle mass and the lowest functional decline risk.
Journal of Gerontology Biological Science and Medical Science 2017: High protein foods and physical activity protect against age-related muscle loss and functional decline [nutritional epidemiology study; very weak evidence]
Subjects ages 70 to 79 eating more protein lost 40% less muscle mass compared to those who ate less:
American Journal of Clinical Nutrition 2008: Dietary protein intake is associated with lean mass change in older, community-dwelling adults: the Health, Aging, and Body Composition (Health ABC) Study
[nutritional epidemiology study with HR<2; very weak evidence]One randomized trial and a large observational study report better bone health in those who ate more protein.
Journal of Bone and Mineral Research 2011: A real and volumetric bone mineral density and geometry at two levels of protein intake during caloric restriction: a randomized, controlled trial
[ moderate evidence]Journal of Bone and Mineral Research 2000:
Effect of dietary protein on bone loss in elderly men and women: the Framingham Osteoporosis Study [nutritional epidemiology study with HR<2; very weak evidence]The following observational study reports a significantly increased risk of dying after a hip fracture.
American Journal of Epidemiology 1993:
↩
Population-based study of survival after osteoporotic fractures [observational study, weak evidence]Protein and satiety
American Journal of Clinical Nutrition 2008: Protein, weight management, and satiety [overview article; ungraded]
Increasing protein from 15% to 30% resulted in a significant caloric drop.
American Journal of Clinical Nutrition 2005: A high protein diet induces sustained reductions in appetite, ad libitum caloric intake, and body weight despite compensatory changes in diurnal plasma leptin and ghrelin concentrations [nonrandomized study, weak evidence]
↩Institute of Medicine of the National Academies 2005: Dietary reference intakes for energy, carbohydrate, fiber, fat, fatty acids, cholesterol, protein, and amino acids [overview article; ungraded]
Journal of the American Dietetic Association 2002: Dietary reference intakes for energy, carbohydrate, fiber, fat, fatty acids, cholesterol, protein and amino acids [overview article; ungraded]
Controversy exists about how they derived the upper limit, as it uses nitrogen balance and is not based on clinical outcomes; it is therefore theoretical and could be even higher.
Journal of Nutrition 2003: Amino acid pharmacokinetics and safety assessment [overview article; ungraded]
Based on calculations of the liver and kidney’s ability to safely handle protein, a 176-pound (80-kilo) person has a theoretical maximum of 365 grams of protein per day. That’s 73% of a 2,000 calorie diet! It’s safe to say that most people won’t have to worry about eating too much protein.
International Journal of Sports Nutrition and Exercise Metabolism 2006: A review of issues of dietary protein intake in humans [overview article; ungraded]
↩“Reference body weight” is a rough approximation of your lean body mass – the part that needs protein. You can look up your reference body weight here or use the simple chart below to estimate your protein needs. ↩
In this case, height is a proxy for reference body weight. Reference body weight is a way of estimating how much lean body mass a person of a specific height would have and thus how much protein they need on a daily basis. ↩
How do you know if you are getting 100 grams? You could estimate that your protein needs are the same as two palms full of protein foods per meal for three meals per day, or you could estimate protein content by the “rule of seven” — meaning every ounce of protein-containing food has about seven grams of protein. These methods are obviously not as accurate as counting and weighing everything you eat, but they may provide a framework for those who don’t want to count (and we don’t blame you if you don’t like counting everything you eat!) ↩
Read more about the unproven links between red meat and cancer in our guide on red meat and our guide on diet and cancer.
The following observational study found the opposite effect — vegetarians had a higher cancer rate than meat-eaters. Since this was a weak nutritional epidemiology study, it doesn’t prove anything. However, it does raise the question of whether there can be dietary variables, more important than red meat consumption, that contribute to the risk of cancer.
American Journal of Clinical Nutrition 2009:
Cancer incidence in vegetarians: results from the European Prospective Investigation into Cancer and Nutrition (EPIC-Oxford) [nutritional epidemiology study with HR<2; very weak evidence] ↩One study reports no harmful effects to kidney and bone health after one year of eating a diet providing 3 grams of protein per kilo of body weight per day. Journal of Nutrition and Metabolism 2016: A high protein diet has no harmful effects: A one-year crossover study in resistance-trained males [randomized trial; moderate evidence]
And the following meta-analysis of nine RCTs and a large observational study both report that those who ate higher amounts of protein had a significantly reduced risk of developing kidney disease. British Journal of Nutrition 2016: Impact of low-carbohydrate diet on renal function: a meta-analysis of over 1000 individuals from nine randomised controlled trials [systematic review of randomized trials; strong evidence]
American Journal of Clinical Nutrition 2021: Causal effects of relative fat, protein, and carbohydrate intake on chronic kidney disease: a Mendelian randomization study [nonrandomized study, weak evidence] ↩
It was thought that acidosis caused a loss of calcium from bone. But it is now recognized that the increase in urinary calcium excretion seen with high protein diets is likely due to increased intestinal absorption of calcium, as opposed to loss of calcium from bone.
Hormone Molecular Biology and Clinical Investigation 2016:
The dietary protein, IGF-I, skeletal health axis[overview article; ungraded]European Journal of Clinical Nutrition 2012: Protein intake, calcium balance and health consequences[overview article; ungraded] ↩
A 2019 meta-analysis reports that a high protein intake (greater than current recommended levels of 0.8 grams per kilo of body weight per day) may be beneficial for the maintenance of bone health and the prevention of bone loss in older adults. Computational and Structural Biotechnology Journal 2019: High versus low dietary protein intake and bone health in older adults: a systematic review and meta-analysis [meta-analysis of randomized controlled trials; strong evidence] ↩
The suggested mechanism for this is that amino acids are known to be used in the production of glucose via gluconeogenesis. However, well-conducted human trials show that dietary protein is not a meaningful contributor to blood glucose in healthy individuals or those with type 2 diabetes (for important information about type 1 diabetes, see further below in this footnote). Even a meal with 50 grams of protein didn’t cause a significant increase in blood sugar in people with diabetes.
Diabetes 2013: Dietary proteins contribute little to glucose production, even under optimal gluconeogenic conditions in healthy humans. [nonrandomized trial; weak evidence]
Journal of Clinical Endocrinology and Metabolism 2001: Effect of protein ingestion on the glucose appearance rate in people with type 2 diabetes [randomized trial; moderate evidence]
The trials included in this review of RCTs did not restrict protein intake and showed significant improvement in blood glucose levels and metabolic health.
BMJ Open Diabetes Research and Care: Systematic review and meta-analysis of dietary carbohydrate restriction in patients with type 2 diabetes [strong evidence]
For people with type 1 diabetes, it is important to note that protein has been found to increase late post-meal blood sugars when consumed along with dietary carbohydrate. In the absence of dietary carbohydrate, protein amounts up to 50 grams do not seem to raise post-meal blood glucose, while 75-100 grams of pure protein can raise blood glucose in a similar fashion to 20 grams of carbohydrate.
Diabetes Care 2015: Impact of fat, protein, and glycemic index on postprandial glucose control in type 1 diabetes: implications for intensive diabetes management in the continuous glucose monitoring era [systematic review; strong evidence] ↩
Two studies report that a diet with 30% of calories from protein improved blood sugar control, and protein has been shown to lower blood glucose to healthy levels in other studies of people with type 2 diabetes.
Diabetes 2004: Effect of a high-protein, low-carbohydrate diet on blood glucose control in people with type 2 diabetes [randomized trial; moderate evidence]
American Journal of Clinical Nutrition 2003: An increase in dietary protein improves the blood glucose response in persons with type 2 diabetes [randomized trial; moderate evidence]
Diabetes Care 2006: Protein hydrolysate/leucine co-ingestion reduces the prevalence of hyperglycemia in type 2 diabetic patients [randomized trial; moderate evidence]
Protein may slightly increase insulin concentrations acutely, but high protein diets are not known to cause hyperinsulinemia (chronically elevated insulin levels).
Diabetes care 2003: Amino acid ingestion strongly enhances insulin secretion in patients with long-term type 2 diabetes. [nonrandomized trial; weak evidence] ↩
EBioMedicine 2019: The impact of dietary protein intake on longevity and metabolic health
[overview article; ungraded] ↩Food and Agriculture Organization of The UNited Nations 2011: Dietary protein quality evaluation in human nutrition [overview article; ungraded]
Amino Acids 2018: Protein content and amino acid composition of commercially available plant-based protein isolates [laboratory study; ungraded]
↩Although the quality of protein in different legumes varies, many appear to be about 20-50% less digestible than animal protein:
Food Science and Nutrition 2017: Determination of the protein quality of cooked Canadian pulses [mechanistic study; ungraded] ↩
One small randomized crossover trial in 20 people, comparing a 30% protein diet from soy protein to an equivalent amount of animal protein, reports no difference in weight loss after two weeks.
American Journal of Clinical Nutrition 2014: Appetite control and biomarkers of satiety with vegetarian (soy) and meat-based high protein diets for weight loss in obese men: a randomized crossover trial
[ moderate evidence]And another shows similar anabolic effects for soy and whey protein supplements.
International Journal of Environmental Research and Public Health 2020: No significant differences in muscle growth and strength development when consuming soy and whey protein supplements matched for leucine following a 12 week resistance training program in men and women: a randomized trial
[ moderate evidence]
↩The following reviews highlight how animal protein has more anabolic (or muscle-building) effects than plant-based protein, concluding: “For example, proteins found in milk, whey, egg, casein, and beef have the highest score (1.0), while scores for plant-based proteins are as follows: soy (0.91), pea (0.67), oat (0.57), and whole wheat (0.45)”
Proceedings of the Nutrition Society 2018: Characterising the muscle anabolic potential of dairy, meat and plant-based protein sources in older adults [overview article; ungraded]
Journal of Nutrition 2015: The skeletal muscle anabolic response to plant – versus animal-based protein consumption [overview article; ungraded]
Nutrition Bulletin 2012: Micronutrient challenges across the age spectrum: Is there a role for red meat? [overview article; ungraded]
↩The following are low-quality nutritional epidemiology studies that suggest a minimal increased risk with red meat intake or a lower risk with eating plant protein. However, as we discuss in our guide on observational vs. experimental studies, this line of evidence is complicated by healthy user bias, poor data collection, confounding variables, and other methodological weaknesses.
JAMA Internal Medicine 2016: Association of animal and plant protein intake with all-cause and cause-specific mortality
[nutritional epidemiology study with HR<2; very weak evidence]British Journal of Nutrition 2014: Association between total, processed, red and white meat consumption and all-cause, CVD and IHD mortality: a meta-analysis of cohort studies [observational study with HR < 2; very weak evidence]
Journal of the American Heart Association 2017. Role of total, red, processed, and white meat consumption in stroke incidence and mortality: A systematic review and meta‐analysis of prospective cohort studies [observational study with HR < 2; very weak evidence]
The following observational study reports that eating more animal protein, but not plant protein, is associated with a higher risk of death in people ages 50 to 65. The same correlation did not hold for those older than 65 years old.
However, the people who chose plant sources of protein had a much lower incidence of diabetes at baseline compared to the higher protein group (2% vs. 17%). Since the main mortality difference was diabetes mortality, the increased risk may have had more to do with underlying health conditions than the protein in their diet.
Cell Metabolism 2014: Low protein intake is associated with a major reduction in IGF-1, cancer, and overall mortality in the 65 and younger but not older population
[nutritional epidemiology study and animal study; very weak evidence]
↩American Journal of Clinical Nutrition 2016:
Mortality in vegetarians and comparable nonvegetarians in the United Kingdom [nutritional epidemiology study; very weak evidence]American Journal of Clinical Nutrition 2009:
Mortality in British vegetarians: results from the European Prospective Investigation into Cancer and Nutrition (EPIC-Oxford) [nutritional epidemiology study; very weak evidence]European Heart Journal 2021:
Vegetarians, fish, poultry, and meat-eaters: who has higher risk of cardiovascular disease incidence and mortality? A prospective study from UK Biobank [nutritional epidemiology study; very weak evidence]
↩