The complete guide to ketosis
Ketosis is a metabolic state in which your body uses fat as its main energy source.
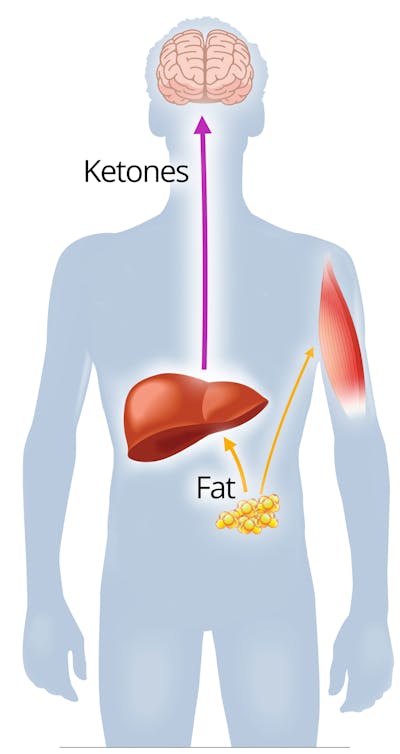
Normally, the body uses glucose, or sugar, as its primary fuel. When carb intake is very low, your liver produces lots of ketones, which are fat-like compounds that your brain and other organs can use in place of glucose.
Being in ketosis may help you feel less hungry, promote weight loss, and possibly provide other benefits.
Read on to learn all you need to know about ketosis, including tips for successfully getting into ketosis and staying there.
Three key takeaways
What is ketosis?Ketosis is a metabolic state in which your body uses fat as its main fuel. Learn more
What are the benefits of ketosis?
Potential benefits include appetite suppression, weight loss, and type 2 diabetes reversal. Learn more
How can I get into ketosis?
To get into ketosis, eat fewer than 20 grams of net carbs per day, eat less often, and don’t fear fat. Learn more
1. What is ketosis?
Ketosis is a metabolic state in which your body uses fat and ketones rather than glucose (sugar) as its main fuel source.
Glucose is stored in your liver and released as needed for energy. However, after carb intake has been extremely low for one to two days, these glucose stores become depleted.1 Your liver can make some glucose from amino acids, glycerol, and lactate via a process known as gluconeogenesis, but not nearly enough to meet all the needs of your brain, which requires a constant fuel supply.2
Fortunately, ketosis can provide you, and especially your brain, with an alternative source of energy.
Ketones, or ketone bodies, are made by your liver from fat that you eat as well as from your own body fat. The three ketone bodies are beta-hydroxybutyrate (BHB), acetoacetate, and acetone (although acetone is technically a breakdown product of acetoacetate).3
Your liver produces ketones on a regular basis even when eating a higher-carb diet. This happens mainly overnight while you sleep but only in tiny amounts. However, when glucose and insulin levels decrease, such as on a carb-restricted diet, the liver ramps up its production of ketones in order to provide energy for your brain.
Once the level of ketones in your blood reaches a certain threshold, you are considered to be in nutritional ketosis. According to leading ketogenic diet researchers Dr. Steve Phinney and Dr. Jeff Volek, the threshold for nutritional ketosis is a minimum of 0.5 mmol/L of BHB (the ketone body measured in blood).4
Although both fasting and a keto diet will allow you to achieve ketosis, only a keto diet is sustainable over long periods of time. In fact, it appears to be a healthy way to eat that people can potentially follow indefinitely.5
Learn more about the keto diet
For more about the keto diet, check out this guide: A ketogenic diet for beginners and the videos below.
- MEMBERS ONLY
![Eating keto to survive cancer]()
![All things keto with Keto Connect]()
- MEMBERS ONLY
![Exploiting cancer metabolism with ketosis]()
![My success story with Jim Caldwell]()
- MEMBERS ONLY
![A new life with a keto diet]()
- MEMBERS ONLY
![Treating cancer with a keto diet]()
- MEMBERS ONLY
![LCHF and diabetes: science and clinical experience]()
![Diet Doctor Podcast #35 with Ben Bikman, PhD]()
- MEMBERS ONLY
![A life without migraines]()
- MEMBERS ONLY
![Challenging the dogma]()
- MEMBERS ONLY
!["I'll do this or I'm going to die trying"]()
- MEMBERS ONLY
![80 pounds lighter and no medications]()
![Diet Doctor Podcast #31 – Dr. Ken Berry]()
- MEMBERS ONLY
![Low-carb living]()
![My success story with Gillian Szollos]()
- MEMBERS ONLY
![Q&A with Miriam Kalamian]()
- MEMBERS ONLY
![Is lower insulin the key to better brain health?]()
- MEMBERS ONLY
![Trouble shooting high blood-glucose levels]()
- MEMBERS ONLY
![How to reverse type 2 diabetes]()
- MEMBERS ONLY
![Can you treat cancer with low carb?]()
- MEMBERS ONLY
![Is fear of protein the new fear of fat?]()
- MEMBERS ONLY
![Low-carb living]()
- MEMBERS ONLY
![How to formulate a low-carb keto diet]()
- MEMBERS ONLY
![Low-carb ketogenic diets for athletes]()














Does the brain need carbs?
There’s a long-standing yet misguided belief that carbs are necessary for proper brain function. In fact, if you ask some dietitians how many carbs you should eat, they’ll likely respond that you need a minimum of 130 grams per day to ensure that your brain has a steady supply of glucose.
However, this isn’t the case. In fact, your brain will remain healthy and functional even if you don’t eat any carbs at all.
Although it’s true that your brain has high energy demands and requires some glucose, ketones can provide about 70% of the brain’s needed fuel. The liver provides the remainder of needed energy in the form of glucose, which is made by gluconeogenesis (literally “making new glucose”).6
This system allowed our hunter-gatherer ancestors to go for long periods without eating because they had access to a fuel source at all times: stored body fat.
Being in ketosis doesn’t have any adverse effects on brain function. On the contrary, many people have reported that that they feel sharper mentally when they’re in ketosis.7
Food for thought: Does the brain need carbs?
2. Benefits of ketosis
In addition to providing a sustainable energy source, ketones – and in particular BHB – may help reduce inflammation and oxidative stress, which are believed to play a role in the development of many chronic diseases.8
Indeed, there are several established benefits and potential benefits of being in nutritional ketosis.
Established benefits:
- Appetite regulation: One of the first things people often notice when they’re in ketosis is that they aren’t hungry as often. In fact, research has shown that being in ketosis suppresses appetite.9 Studies also show a decrease in ghrelin, the so-called “hunger hormone.” 10
- Weight loss: Many people naturally eat less when they restrict carbs and are allowed as much fat and protein as they need to feel full. Because ketogenic diets suppress appetite, decrease insulin levels, and increase fat burning, it isn’t surprising that they’ve been shown to either outperform or be equivalent to other diets intended for weight loss.11
- Reversal of diabetes and prediabetes:12 In people with type 2 diabetes or prediabetes, being in ketosis can help normalize blood sugar and improve insulin sensitivity, potentially leading to the discontinuation of diabetes medication.13
- Potentially enhanced athletic performance: Ketosis may provide an extremely long-lasting fuel supply during sustained exercise in both high-level and recreational athletes.14
- Seizure management: Maintaining ketosis with the classical ketogenic diet or less stringent modified Atkins diet (MAD) has been proven effective for controlling epilepsy in both children and adults who don’t respond to anti-seizure medication.15
There is also exciting early research suggesting that ketosis may be beneficial for many other conditions, such as reducing the frequency and severity of migraine headaches, reversing PCOS, perhaps enhancing conventional brain cancer therapies, possibly slowing down the progression of Alzheimer’s disease, along with potentially helping people live longer, healthier lives. Although higher quality research is needed to confirm these effects, much of the early research is very encouraging.
3. Nutritional ketosis vs. ketoacidosis
Nutritional ketosis and diabetic ketoacidosis are entirely different conditions. While nutritional ketosis is safe and beneficial for health, ketoacidosis is a medical emergency.16
Unfortunately, many healthcare professionals don’t really understand the distinction between the two.
Ketoacidosis occurs mainly in people with type 1 diabetes if they aren’t getting enough insulin to meet their needs. In diabetic ketoacidosis (DKA), blood sugar and ketones rise to dangerous levels, which disrupts the blood’s delicate acid-base balance.17
In nutritional ketosis, BHB levels typically remain below 5 mmol/L. However, people in diabetic ketoacidosis often have BHB levels of 10 mmol/L or above, which is directly related to their inability to produce insulin.18
This graph shows the vast difference in the amount of ketones in the blood between ketosis and ketoacidosis:19

Other people who can potentially go into ketoacidosis are those with type 2 diabetes who take medications known as SGLT-2 inhibitors, such as empagliflozin, canagliflozin, dapagliflozin, and ertugliflozin.20
Also, in rare cases, women who don’t have diabetes can develop ketoacidosis while breastfeeding.21
However, for most people capable of producing insulin, it’s nearly impossible to go into ketoacidosis.



4. Tips for getting into ketosis
There are a number of ways you can get into nutritional ketosis safely and effectively.
- Reduce daily net carb intake to less than 20 grams: Although it’s possible that you may not need to be this strict, eating fewer than 20 grams of net carbs every day virtually guarantees that you’ll achieve nutritional ketosis, and is likely the only advice you will need.22 What does 20 grams of carbs look like? Use our visual guide to find out, or simply try our keto recipes and meal plans that limit carbs to less than 20 grams per day.
- Try intermittent fasting: Going for 16-18 hours without eating may help you get into ketosis more quickly.23 This is easy to do by simply skipping breakfast or dinner, which may feel very natural on an appetite-suppressing keto diet.
- Don’t fear fat: Although the main key is reducing carbs, adding calories from fat and protein can help you make the transition to fat burning with less hunger, especially when you are just getting started.24 As you progress on your low-carb journey, it may help to gradually lower your fat intake to ensure you are burning your body fat stores. This doesn’t mean you should eat a low fat diet. It simply means you may not have to purposefully add extra fat when you don’t need the extra calories.
- Cook with coconut oil: In addition to being a natural fat that remains stable at high heat, coconut oil contains medium-chain fatty acids that can boost ketone production and may also have other benefits.25 While it is not a requirement for weight loss, if you are interested in raising your ketones for other reasons, coconut oil can help.
- Exercise, if possible: During the transition into ketosis, you may not have enough energy to engage in vigorous physical activity. However, simply going for a brisk walk may help you get into ketosis more easily.26
Even more tips for how to get into ketosis on a keto diet
Supplements not required
Note what’s not on the list above: you do not need expensive supplements, like exogenous ketones or MCT oil (medium-chain triglycerides). These supplements will likely not help you lose weight or reverse disease. At least there’s no evidence for that.27

Ketone supplements do not lower insulin or blood sugar and don’t increase fat burning.28 It’s hard to believe that they would have any direct benefits for weight loss or type 2 diabetes reversal.29
What these ketone supplements might do is improve mental and physical performance for a short time.30 To the best of our knowledge, this potential is also unproven. They do raise blood levels of ketones, an effect that can last anywhere from one to a few hours.
We’re not saying don’t buy these supplements. Perhaps you want to try them for yourself, and see how they make you feel. But you don’t need them to be successful on a keto diet or to get into ketosis. Here’s our big test of keto supplements:
Exogenous ketone supplements: Do they work?
5. Protein’s effect on ketosis
Although getting sufficient protein on any diet is important for preventing muscle loss, many questions have been raised about protein’s impact on ketone levels.
During digestion, protein is broken down into individual amino acids, which triggers the release of insulin. Although the amount of insulin needed to transport these amino acids into muscles is small, when large amounts of protein are consumed, the rise in insulin might reduce ketone production to some extent.
For this reason, ketogenic diets for epilepsy are restricted in protein as well as carbs, which ensures that ketone levels remain elevated at all times.
However, protein’s effect on ketosis seems to be highly individualized.31
For example, when Diet Doctor’s Bjarte Bakke conducted several “n of 1” experiments to see how much protein he could eat and still remain in ketosis, he found that keeping net carb intake below 20 grams per day was what ultimately mattered regardless of his protein intake.
Clinical experience would suggest that others are likely to have the same results as Bjarte.
If you want to stay in ketosis and still eat plenty of protein and are concerned about potential negative effects, it might be a good idea to conduct your own n of 1 experiments in order to determine your personal protein threshold. It may be higher than you think.
Read more about protein on a ketogenic diet
6. What is optimal ketosis?
Getting into ketosis on a ketogenic diet involves a broad range, and you can achieve different degrees of ketosis. The term “optimal” ketosis is frequently used, but it is poorly defined. For instance, those treating seizures or Alzheimer’s disease may benefit from targeting a ketone level above 1.5 mmol/L, whereas for losing weight or improving blood sugar the degree of elevation may not matter at all. The numbers below refer to values when testing blood ketone levels.32

- Below 0.5 mmol/l is not considered “ketosis,” although a value of, say, 0.2 demonstrates that you’re getting close. At this level, you may not be at your maximum fat-burning zone.
- Between 0.5 – 3 mmol/l is nutritional ketosis. You’ll likely be getting a good effect on your appetite and metabolic improvements.33
- Around 1.5 – 3 mmol/l is called “optimal” ketosis by some. However, the concept of optimal ketosis is controversial, and it’s unclear if it offers any substantial benefits over the 0.5-1.5 level. Exceptions could be treating seizures or those interested in maximum mental and physical performance gains.34
- Over 3 mmol/l is higher than necessary. It will probably achieve neither better nor worse results than being at the 1.5–3 level.35 Higher numbers can also sometimes mean that you’re not getting enough food (“starvation ketosis”).36 In people with type 1 diabetes, ketone levels over 3.0 mmol/L can be caused by a severe lack of insulin that requires urgent medical attention.37
- Over 8–10 mmol/l: It’s normally impossible to get to this level just by eating a keto diet. It means that something is wrong. The most common cause by far is type 1 diabetes, with a severe lack of insulin. Symptoms include feeling very sick with nausea, vomiting, abdominal pain and confusion. The possible end result, ketoacidosis, may be fatal and requires immediate medical care.

7. Signs that you are in ketosis
There are several signs that suggest you’re in ketosis, although measuring your ketones is the only objective way to verify it. Here are the most common signs and symptoms:
- Dry mouth or a metallic taste in the mouth.
- Increased thirst and more frequent urination.
- “Keto breath” or “fruity breath,” which may be more apparent to others than yourself. Learn more
- Initial fatigue, followed by an increase in energy.
- Decrease in appetite and food intake (one of the more welcome side effects!).
Measuring ketones
There are three ways to measure ketones, which all come with pros and cons. For a detailed comparison, see our full guide to the best way to test ketones.
For a shorter version, keep reading below. Note that we have no affiliations with any of the brands mentioned here.38
1. Urine strips![ketostix]()
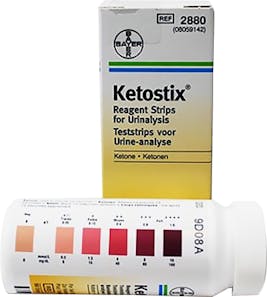
Urine strips are the simplest and cheapest way to measure ketosis. It is the first option for most beginners on a keto diet.
Dip the strip in your urine, and 15 seconds later the color change will show you the presence of ketones.39 If you get a high reading (a dark purple color), you’ll know that you’re in ketosis.
2. Breath-ketone analyzers

Breath-ketone analyzers are a simple way to measure ketones.41 At $236 and up they are more expensive than urine strips. But they are cheaper than blood-ketone meters in the long run, as they are reusable any number of times.
These analyzers vary in their specific results. Some older models do not give you a precise ketone level; rather, they provide a color code for the general level. Whereas other, newer models, report a specific number or level.
3. Blood-ketone meters![Blood ketone meters: Precision extra and Keto-Mojo]()
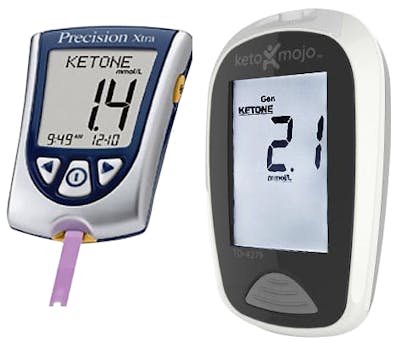
Blood-ketone meters show the exact and current level of ketones in your blood.42 They are the gold standard method for measuring your level of ketosis on a ketogenic diet. They used to be quite expensive, but prices have come down significantly over the years.43
What if you’re not in ketosis?
If you’re on a keto diet but aren’t seeing any signs or symptoms of being in ketosis, here are a few strategies that may help:
- Track your carb intake. While we don’t recommend counting or tracking calories, it can be helpful to log your carb intake to make sure you’re truly eating less than 20 grams of carbs. Use an online site or app, such as Cronometer, Senza, Carb manager, and others.
- Test blood ketones in the late morning or afternoon. Blood and urine ketones vary throughout the day, as well as from person to person.44 Many people find that their blood ketone levels are usually lowest right after waking up.45 Try testing later on, preferably a few hours after eating. Even if you’re only in ketosis for a portion of the day, you’re still getting some benefits, as discussed in this talk by Dr. Steve Phinney: Achieving and maintaining nutritional ketosis.
- Try to be patient. Although some people get into ketosis relatively quickly, it may take others a while.46 Unfortunately, people who are insulin resistant often seem to have a longer journey. Put in a solid month of consistent keto eating, and try to ramp up your physical activity, if possible. Within four weeks, you should definitely be in ketosis and experiencing its benefits.

Which is the best ketone meter on the market?
GuideWith a blood ketone meter, you can test for blood levels of ketones. Here’s our review of the top options.
8. Side effects, fears and potential dangers
Side effects typically happen within the first few days of starting a ketogenic diet and include headache, fatigue, lightheadedness, irritability, cramps, and constipation. These are known collectively as the “keto flu,” which can be remedied by managing fluids and electrolytes, among other things. Read more about the keto flu.
Is being in ketosis safe for everyone?
Being in ketosis is safe for most people, and it can provide many health benefits, including weight loss and reduction of blood glucose and insulin levels, to name a few.
However, certain individuals should only follow a ketogenic diet under medical supervision, and others are best off avoiding it altogether.
Conditions that require medical supervision and monitoring during ketosis:47
- Type 1 diabetes
- Type 2 diabetes on insulin or oral diabetes medications
- High blood pressure on medication
- Liver, heart, or kidney disease
- History of gastric bypass surgery
- Pregnancy
Conditions for which ketosis should be avoided:
- Breastfeeding women
- Individuals with rare metabolic conditions that are typically diagnosed in childhood, such as enzyme deficiencies that interfere with the body’s ability to make and use ketones or to properly digest fats.48

The keto flu, other keto side effects, and how to cure them
GuideDuring the first few days of a keto diet, you can experience the keto flu. You can feel tired, have a headache, and be easily annoyed. Learn all about the keto flu and how to avoid it here.
Recommended viewing



What is ketosis? - the evidence
This guide is written by Franziska Spritzler, RD and was last updated on June 19, 2025. It was medically reviewed by Dr. Michael Tamber, MD on October 9, 2021 and Dr. Bret Scher, MD on October 3, 2022.
The guide contains scientific references. You can find these in the notes throughout the text, and click the links to read the peer-reviewed scientific papers. When appropriate we include a grading of the strength of the evidence, with a link to our policy on this. Our evidence-based guides are updated at least once per year to reflect and reference the latest science on the topic.
All our evidence-based health guides are written or reviewed by medical doctors who are experts on the topic. To stay unbiased we show no ads, sell no physical products, and take no money from the industry. We're fully funded by the people, via an optional membership. Most information at Diet Doctor is free forever.
Read more about our policies and work with evidence-based guides, nutritional controversies, our editorial team, and our medical review board.
Should you find any inaccuracy in this guide, please email andreas@dietdoctor.com.
BBA Clinical 2016: Glycogen metabolism in humans [overview article; ungraded] ↩
It’s estimated that under normal circumstances, the brain requires about 110 to 145 grams of glucose daily to function properly:
Journal of Clinical Investigation 1967: Brain metabolism during fasting [non-controlled study; weak evidence] ↩
The physiology of ketone production and utilization has been well-described in the medical literature. Below are 3 review articles that expand into more detail about the process:
Diabetes and Metabolism Reviews 1989: Ketone body production and disposal: effects of fasting, diabetes, and exercise. [overview article; ungraded]
Annual Reviews in Biochemistry 1980: Regulation of hepatic fatty acid oxidation and ketone body production. [overview article; ungraded]
Annual Reviews in Nutrition 2006: Fuel metabolism in starvation. [overview article; ungraded] ↩
Dr. Phinney and Dr. Volek discuss the range of nutritional ketosis in pages 4-5 of their book The Art and Science of Low Carbohydrate Performance. This is based mostly on their clinical experience, and some may argue that even lower BHB levels may still represent adequate nutritional ketosis.
As a reminder, we may link to books and products such as the book above, but Diet Doctor will not benefit from your purchases. We do not show ads, use any affiliate links, sell products or take money from industry. Instead we’re funded by the people, via our optional membership. Learn more ↩
The main fear about lower-carb and higher-fat diets has been a possible increase in the risk of heart disease. However, interventional studies so far indicate that on average, most cardiovascular risk factors appears to improve:
British Journal of Nutrition 2016: Effects of low-carbohydrate diets v. low-fat diets on body weight and cardiovascular risk factors: a meta-analysis of randomised controlled trials. [strong evidence for improved risk factors]
PLoS One 2015: Dietary intervention for overweight and obese adults: comparison of low-carbohydrate and low-fat diets. A meta-analysis. [strong evidence for improved risk factors]
Obesity reviews 2012: Systematic review and meta‐analysis of clinical trials of the effects of low carbohydrate diets on cardiovascular risk factors [strong evidence for improved risk factors]
American Journal of Clinical Nutrition 2021: Effects of a low-carbohydrate diet on insulin-resistant dyslipoproteinemia-a randomized controlled feeding trial[randomized trial; moderate evidence]
Circulation 2010: Dietary intervention to reverse carotid atherosclerosis [moderate evidence for a reduction in atherosclerosis] ↩
Journal of Clinical Investigation 1967: Brain metabolism during fasting [non-controlled study; weak evidence]
The Journal of Clinical Investigation 1966: Hormone-fuel interrelationships during fasting [non-controlled study; weak evidence] ↩
This is mostly based on [anecdotal reports; very weak evidence]
However, one study showed improved neurocognitive function in AIDS patients when consuming a ketogenic diet:
Journal of the Association of Nurses AIDS Care. 2019: Cognitive effects of a ketogenic diet on neurocognitive impairment in adults aging with HIV: A pilot study. [Small, Pilot RCT; weak evidence]
↩Diabetes Research and Clinical Practice 2015: β-hydroxybutyrate: Much more than a metabolite [overview article; ungraded]
Nature and Medicine 2015: The ketone metabolite β-hydroxybutyrate blocks NLRP3 inflammasome-mediated inflammatory disease [overview article; ungraded]
↩Obesity Review 2015: Do ketogenic diets really suppress appetite? A systematic review and meta-analysis [systematic review of randomized trials; strong evidence] ↩
One study looked at people who lost weight by following a ketogenic diet for eight weeks and then reintroduced small amounts of carbs. The researchers reported that levels of ghrelin were suppressed in those who remained in ketosis, whereas those who were no longer in ketosis had higher ghrelin levels:
European Journal of Clinical Nutrition 2013: Ketosis and appetite-mediating nutrients and hormones after weight loss [non-controlled study; weak evidence] ↩
PLoS One 2015: Dietary intervention for overweight and obese adults: Comparison of low-carbohydrate and low-fat diets. A meta-analysis [strong evidence] Learn more
Journal of Medical Internet Research 2017: An online intervention comparing a very low-carbohydrate ketogenic diet and Lifestyle recommendations versus a plate method diet in overweight individuals with type 2 diabetes: a randomized controlled trial [randomized trial; moderate evidence]
 
Diabetes & Metabolic Syndrome 2017: Induced and controlled dietary ketosis as a regulator of obesity and metabolic syndrome pathologies [randomized trial; moderate evidence]
↩Some disagree with the use of the word “reverse” when it comes to type 2 diabetes. The concern is that it may imply the disease is completely gone, never to return. At Diet Doctor, we use the term “reverse” to indicate that blood sugars are no longer in the diabetic range. However, we acknowledge that blood glucose will likely return to diabetic levels if a patient goes back to their prior high-carb eating habits. Therefore, “reverse” does not imply a forever cure. ↩
Nutrients 2020: Impact of a ketogenic diet on metabolic parameters in patients with obesity or overweight and with or without type 2 diabetes: A meta-analysis of randomized controlled trials [systematic review of randomized trials; strong evidence]
Nutrition & Metabolism (London) 2005: A low-carbohydrate, ketogenic diet to treat type 2 diabetes [non-controlled study; weak evidence]
Frontiers in Endocrinology 2019: Long-term effects of a novel continuous remote care intervention including nutritional ketosis for the management of type 2 diabetes: A 2-year non-randomized clinical trial [weak evidence] ↩
Extreme Physiology & Medicine 2014: Acute nutritional ketosis: implications for exercise performance and metabolism [overview article; ungraded]
However, not all studies show improved athletic performance, The following study showed a decrease in 30km race-walking performance after 12-weeks of a ketogenic diet. Some argue a longer adaptation period is required for improved performance.
PLOS One 2020:Crisis of confidence averted: Impairment of exercise economy and performance in elite race walkers by ketogenic low carbohydrate, high fat (LCHF) diet is reproducible [randomized trial; moderate evidence]
Nutritional Neuroscience 2017: Short-term and long-term efficacy of classical ketogenic diet and modified Atkins diet in children and adolescents with epilepsy: A systematic review and meta-analysis. [systematic review of randomized trials; strong evidence]
Journal of Clinical Neurology 2015: Efficacy of and patient compliance with a ketogenic diet in adults with intractable epilepsy: a meta-analysis [systematic review of randomized trials; strong evidence] ↩
Nutrition Bulletin 2011: Ketosis, ketoacidosis and very-low-calorie diets: Putting the record straight [overview article; ungraded] ↩
People in ketoacidosis feel extremely ill and experience profound dehydration, vomiting, abdominal pain, and weakness. DKA requires hospitalization so that IV fluids and insulin can be given to gradually and safely lower blood sugar.
American Family Physician 2013: Diabetic ketoacidosis: Evaluation and treatment [overview article; ungraded] ↩
When blood ketone levels rise beyond a certain level, a pancreas capable of making insulin will release enough to shut down further ketone production. By contrast, the pancreas of a person with type 1 diabetes cannot make insulin. So unless insulin is given via injection or IV, ketones will continue rising to life-threatening levels.
Diabetes Metabolism Research & Reviews 1999: Ketone bodies: a review of physiology, pathophysiology and application of monitoring to diabetes[overview article; ungraded]
↩This graph denotes an “optimal ketosis” zone between 1.5mmol/L and 3.0mmol/L. Although strong evidence is lacking, clinical experience suggests that targeting this zone may be beneficial for people who are treating neurological or psychiatric conditions such as Alzheimer’s disease, bipolar disorder, or others. However, for general health and weight loss, it is likely less important to target specific ketone levels. ↩
Reviews on Recent Clinical Trials 2018: Diabetic ketoacidosis in patients with type 2 diabetes on sodium-glucose cotransporter-2 inhibitors – a case series [weak evidence] ↩
Case Reports in Nephrology: Ketogenic diet-induced severe ketoacidosis in a lactating woman: a case report and review of the literature [very weak evidence] ↩
Nutrition X 2019: Effects of differing levels of carbohydrate restriction on the achievement of nutritional ketosis, mood, and symptoms of carbohydrate withdrawal in healthy adults: A randomized clinical trial [randomized trial; moderate evidence] ↩
This is based on consistent clinical experience of low-carb practitioners. [weak evidence] ↩
This is based on the consistent clinical experience of practitioners familiar with low-carb nutrition. [weak evidence] ↩
The Journal of Nutrition and Metabolism 2018: The effect of medium chain triglycerides on time to nutritional ketosis and symptoms of keto-induction in healthy adults: a randomised controlled clinical trial [randomized trial; moderate evidence]
 
British Journal of Nutrition 2015: The role of dietary coconut for the prevention and treatment of Alzheimer’s disease: potential mechanisms of action [overview article; ungraded] ↩This is based on anecdotal reports from people following ketogenic diets.[very weak evidence] ↩
As far as we know there are no high-quality studies (RCTs) that test these supplements and determine their health effects, beyond raising ketone levels. Here is a recent review:
PeerJ 2018: The use of nutritional supplements to induce ketosis and reduce symptoms associated with keto-induction: a narrative review [overview article; ungraded]
Exogenous ketone supplements do raise ketone levels in the blood:
Frontiers in Physiology 2017: On the metabolism of exogenous ketones in humans [moderate evidence for raising ketone levels]
One study of MCT oil for mild cognitive impairment is sometimes mentioned, but it did not show any clear effect. Out of only six participants two quit during the study, one saw some improvement and one got worse:
BBA Clinical 2015: Pilot feasibility and safety study examining the effect of medium chain triglyceride supplementation in subjects with mild cognitive impairment: A randomized controlled trial [very weak evidence] ↩
As far as we know there is no good reason to believe that exogenous ketones could have these effects and no studies demonstrating it. ↩
An indirect benefit could be possible – if the supplements result in less hunger, they could reduce food intake and potentially aid weight loss. This theory would have to be tested, and as far as we know it has not been tested. ↩
Some also have concerns about protein’s effect on blood sugar. Thus far, the scientific literature does not support the concern that too much protein worsens blood sugar control for most individuals. For instance, three studies showed a diet with 30% of calories from protein improved glycemic control.
American Journal of Physiology, Endocrinology, and Metabolism 2020: Effects of carbohydrate restriction on postprandial glucose metabolism, beta-cell function, gut hormone secretion, and satiety in patients with type 2 diabetes [randomized trial; moderate evidence]
Diabetes 2004: Effect of a high-protein, low-carbohydrate diet on blood glucose control in people with type 2 diabetes [randomized trial; moderate evidence]
American Jopurnal of Clinical Nutrition 2003: An increase in dietary protein improves the blood glucose response in persons with type 2 diabetes [randomized trial; moderate evidence]
And another study found patients with type 2 diabetes eating a 50g protein meal had no significant increase in serum glucose concentration.
Journal of Clinical Endocrinology and Metabolism 2001: Effect of protein ingestion on the glucose appearance rate in people with type 2 diabetes [randomized trial; moderate evidence] ↩
The chart is from the book The Art and Science of Low-Carbohydrate Performance by Professor Stephen Phinney and Jeff Volek. However, these definitions of ketone ranges aren’t based on clinical trials but rather a compilation of clinical opinion.
This graph denotes an “optimal ketosis” zone between 1.5mmol/L and 3.0mmol/L. Although strong evidence is lacking, clinical experience suggests that targeting this zone may be beneficial for people who are treating neurological conditions such as Alzheimer’s disease, bipolar disorder, or others. However, for general health and weight loss, it is likely less important to target specific ketone levels.
The levels of the fat-storing hormone insulin will probably be relatively low, as low insulin levels are normally required for ketosis. ↩
The scientific evidence for the mental and physical benefits of this is not strong. Even though 1.5-3.0 mmol/L is considered “optimal” by some, achieving this BHB level isn’t necessary for weight loss and blood glucose control. ↩
This is based on the clinical experience and research of low-carb practitioners. [weak evidence] ↩
Sustained levels above 3.0 or 4.0 mmol/L may occasionally occur in some people following a ketogenic diet, but they’re more often seen in starvation ketosis, which occurs after fasting for several days. ↩
Seek immediate medical attention if you have type 1 diabetes and experience ketone levels over 3.0 mmol/L. ↩
At Diet Doctor we show no ads, sell no products and take no money from industry. Neither do we use any affiliate links or profit in any way from the products we mention.
We’re fully financed by the people, via our optional membership. Learn more ↩
The strips measure the ketone acetoacetate. The presence of this in your urine indicates that you’ve been in ketosis during the hours before testing. ↩
Diabetes 1985: Ketone body production and disposal in diabetic ketosis: a comparison with fasting ketosis [non-randomized study; weak evidence] ↩
Breath analyzers measure the ketone acetone. ↩
Blood-ketone meters measure the ketone beta-hydroxybutyrate (BHB). ↩
A meter with 10 ketone-test strips included now runs about $40-50, with additional strips costing about $1 each. ↩
One study found that urine ketone levels tended to be highest in the morning and after dinner:
Nutrition and Metabolism 2014: Monitoring for compliance with a ketogenic diet: what is the best time of day to test for urinary ketosis? [non-controlled study; weak evidence] ↩
This is based on consistent clinical experience of low-carb practitioners. [weak evidence] ↩
This is based on consistent clinical experience of low-carb practitioners. [weak evidence] ↩
These recommendations are based on clinical expertise and level of clinical concern and, therefore, this list may not be all-inclusive. ↩
Department of Neurology 2012: Chapter 45 – Ketogenic diet [textbook chapter; ungraded] ↩