

Evidence based
How to improve and measure your body composition
You may have started a new diet and exercise program and feel you are making progress. But when you step on the scale, nothing has changed. Does that mean your efforts “aren’t working?”Not necessarily.
Or, maybe your doctor tells you that your body mass index (BMI) is high. Do you know what that means, and is it necessarily bad news?
It depends.
The scale and BMI are rudimentary tools for gauging your overall body composition, meaning they don’t tell you enough to determine if you are at a healthy weight.
Here’s an example. A professional athlete may be six feet tall (183 cm), weigh 225 pounds (102 kg), and be in fantastic physical condition with a 32-inch waist (81 cm) and bulging muscles. A busy doctor may be six feet tall and weigh 225 pounds with a 39-inch waist (99 cm) and a bulging midsection.
They have the same weight and the same BMI, but very different health assessments. What’s different? The two men have different amounts of muscle tissue and fat mass. The athlete has a healthy body composition. The doctor perhaps does not.
Knowing your body composition gives you a better picture of your overall health than just knowing weight or BMI.
Key takeaways
Improving your body composition means eliminating excess fat mass and increasing lean mass by building muscle, which helps improve metabolic health parameters like blood sugar, insulin resistance, and blood pressure.Sustainably decreasing caloric intake is the best way to reduce fat mass, and resistance training is likely the best form of exercise for building muscle mass.
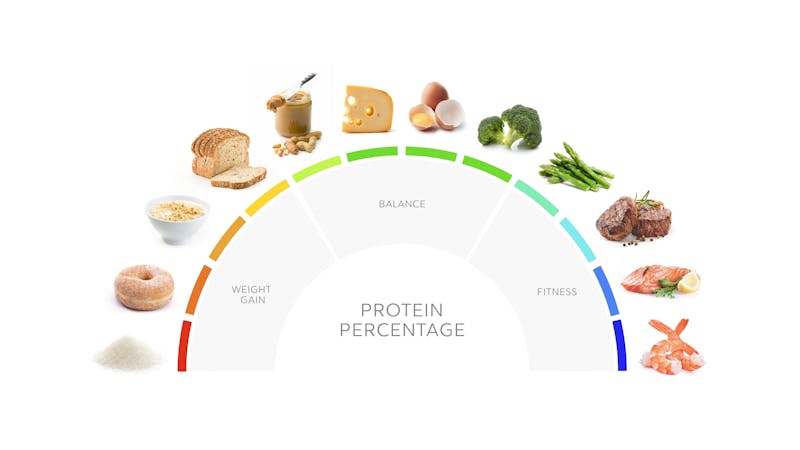
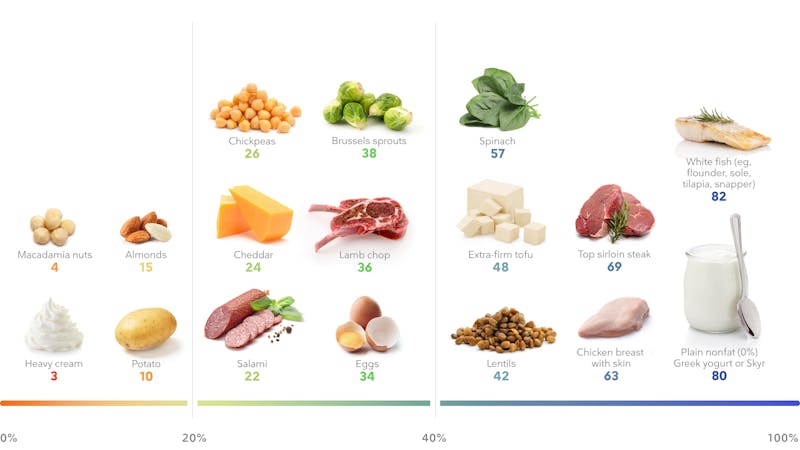
Higher protein diets help you maximize body composition improvement from resistance training.


Low carb recipes








Short-term intermittent fasting for fat loss
Time-restricted eating or short-term intermittent fasting, of less than 36 hours, can help with fat-mass loss with minimal to no loss of muscle mass. However, with longer fasting periods, there is a concern about losing muscle mass.
One study shows that six weeks of alternate-day fasting led to a 7% overall weight loss, most of it fat mass.
Another randomized trial reports more significant fat-mass loss with intermittent calorie restriction than with traditional dieting.
And an analysis of eight studies looking at time-restricted eating or alternate-day fasting plus resistance training demonstrates maintenance or even an increase in muscle mass.
Although not all studies agree. For instance, one randomized controlled trial that did not dictate how much or what the subjects ate didn’t demonstrate a benefit for lean mass in those doing 16:8 time-restricted eating.
Older studies with longer fasting periods report a negative nitrogen balance — a marker of muscle loss.
What should we make of this evidence? Time-restricted eating and short-term intermittent fasting may help reduce calories without significant muscle-mass loss. But longer fasts may lead to muscle-mass loss, and what you eat during your “eating window” may impact your body-composition response. Given the limited amount of research in this field, we need studies that assess the long-term effects of intermittent fasting on body composition.
What to avoid to improve body composition
When looking to improve your body composition, what you don’t eat may be just as important as what you do eat. Here are three things to avoid to improve your body composition.

Alcohol provides calories without nutrition which can make it difficult to sustainably reduce caloric intake. In addition, alcohol can diminish inhibitions and self control, leading to excessive calorie consumption.

Sugar provides calories without nutrition and stimulates the brain’s reward center, encouraging you to eat more and stimulating your cravings.

Engineered foods like chips, crackers, and treats are designed to make you want more. They tend to be high in fat and carbs, with little protein or nutrition. Their satiety index is very low, and thus you can easily overeat them.
Summary
High protein diets are most beneficial for adding muscle mass. High protein, low carb diets are also beneficial for losing fat mass and improving satiety.Other dietary approaches that reduce calories, including intermittent fasting, may also improve body composition, but too much calorie restriction for too long may negatively impact muscle mass.
Exercise
In addition to proper nutrition, exercise can be a powerful tool for improving body composition. Here’s what science has to say about the best exercises.